Engineered for precision. Explore our top-tier catalog including orthopedic implant accessories and dynamic surgery instruments.
Understanding the clinical and mechanical benchmarks governing fracture reduction, anatomic alignment, and angular stability.
Distal radius fractures are among the most frequently managed skeletal injuries in orthopedic traumatology, accounting for approximately 17% of all emergency room fracture presentations. The primary clinical objective in treating unstable distal radius fractures is the restoration of anatomical congruency—specifically, restoring radial height (averaging 11-12mm), volar tilt (typically 11 degrees), and radial inclination (around 22 degrees). The introduction of anatomically pre-contoured distal radius volar locking plates has revolutionized this surgical domain, providing stable internal fixation even in severely comminuted osteoporotic bone.
From a biomechanical perspective, distal radius locking plates function as internal fixators. Traditional non-locking systems rely heavily on the friction interface created between the plate and the bone cortex, which can fail under cyclic load in patients with suboptimal bone mineral density. Conversely, locking plate constructs maintain angular stability because the screw heads thread directly into the plate's locking holes. This rigid screw-plate interface transitions the load pathway from the bone-screw interface directly to the plate construct, preventing secondary loss of alignment and maintaining articular reduction during early active mobilization programs.
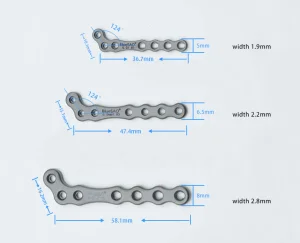
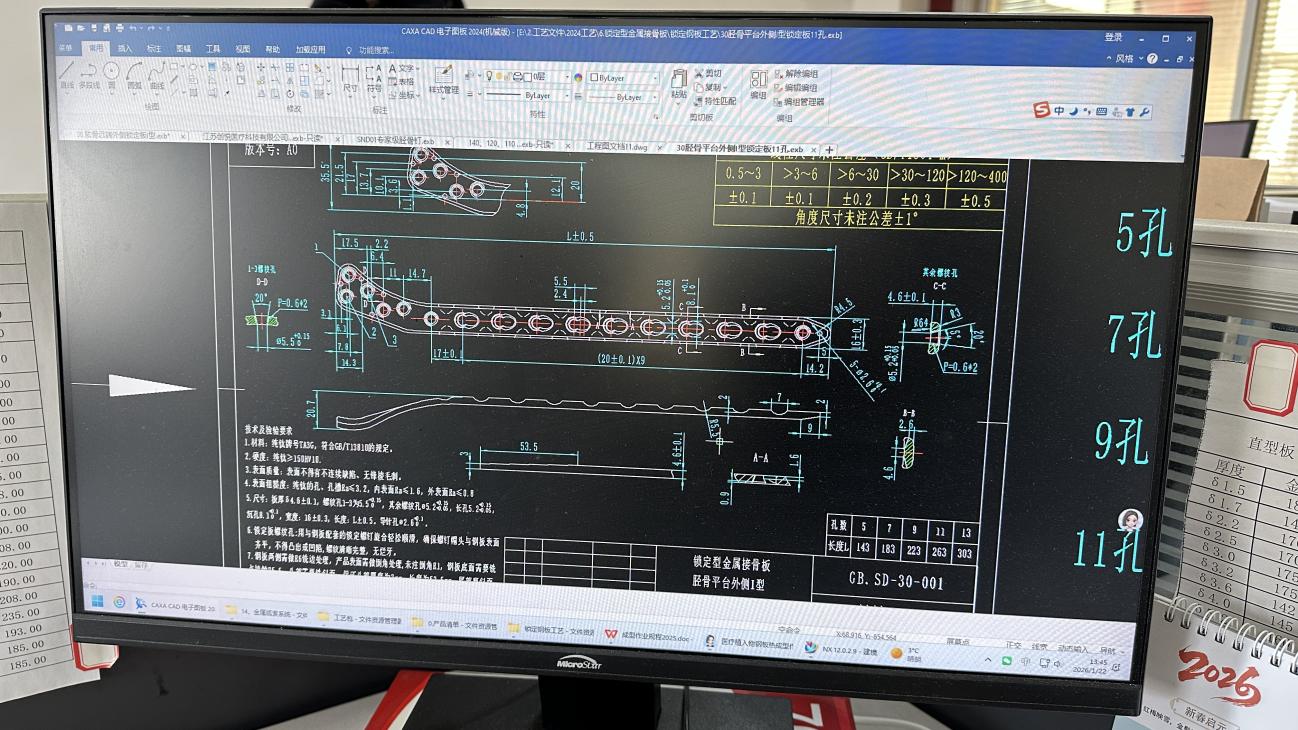
Medical device sourcing directors and clinical purchasing committees must assess the engineering parameters of these implants. Plate thickness profile (typically ranging between 1.5mm to 2.4mm), distal screw trajectories, cluster hole patterns, and material fatigue life are critical factors. Tier-1 manufacturing facilities leverage advanced finite element analysis (FEA) to minimize the risk of stress shielding while simultaneously optimizing the fatigue resistance of the constructs under repetitive physiological loads.
Decentralized supply chains and the rigorous validation framework required for international orthopedic procurement.
Manufacturers must adhere strictly to ISO 13485 quality systems. In the EU, compliance under the Medical Device Regulation (MDR 2017/745) Class IIb/III is mandatory, requiring comprehensive clinical evaluation reports (CERs) and post-market clinical follow-up (PMCF) to ensure long-term implant performance.
Implants must utilize medical-grade titanium alloys such as Ti-6Al-4V ELI (ASTM F136) or pure titanium (ISO 5832-3). These alloys offer exceptional strength-to-weight ratios, high fatigue limits, and superior biocompatibility, minimizing long-term structural failure and adverse tissue reactions.
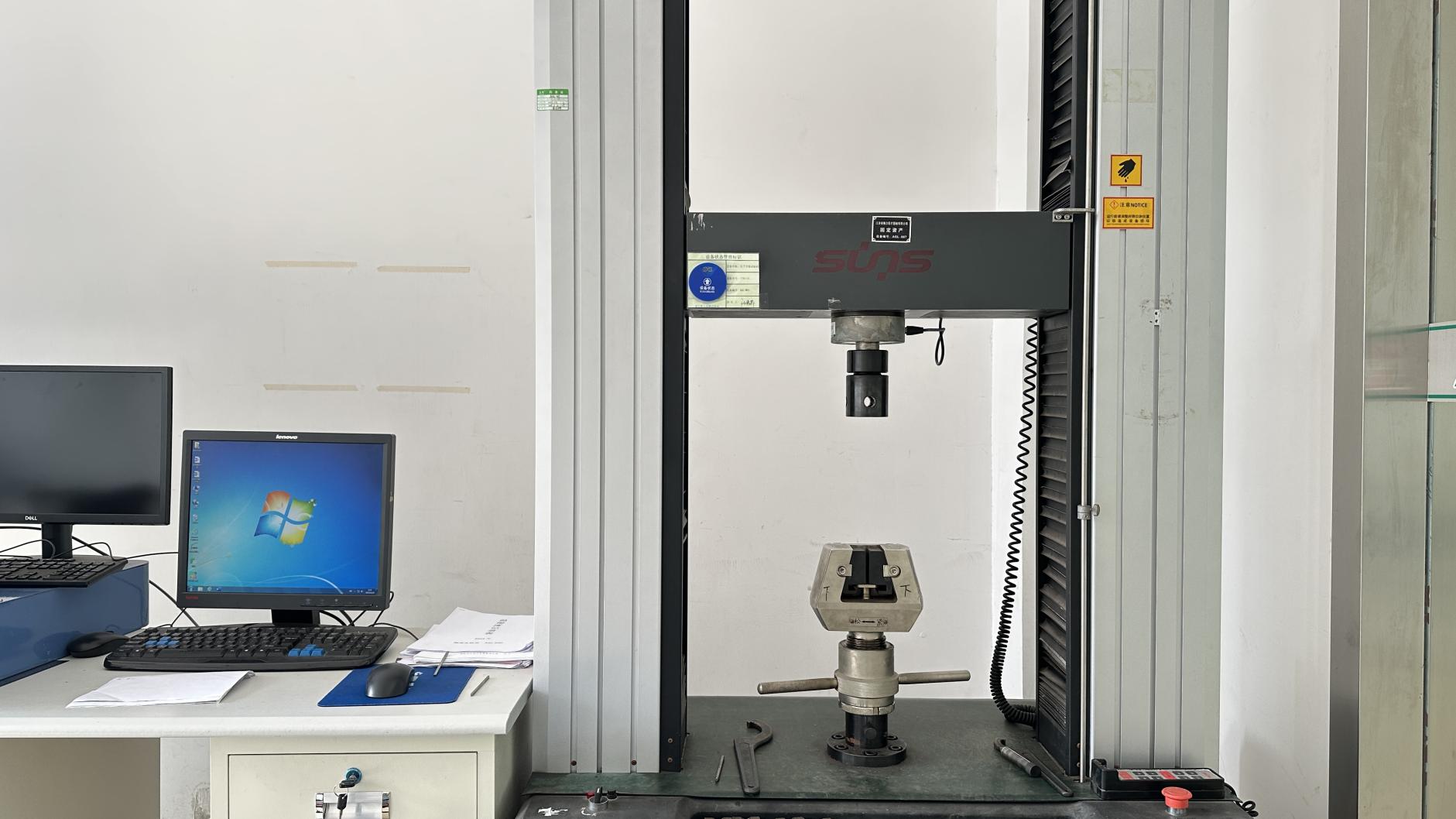
Implants must withstand up to 1 million cycles of mechanical testing without deformation, simulating physiological loads over years of patient movement. Dynamic testing ensures the plate won't fail before complete bone union is achieved.
| Feature / Parameter | Standard Industry Specs | Virelox High-End System Standards | Sourcing Importance for Distributors |
|---|---|---|---|
| Raw Material Origin | ASTM F136 Titanium Alloy | Traceable Titanium Alloys with mill certificates | Prevents catastrophic implant breakage |
| Low Profile Thickness | 2.0mm - 2.5mm | Anatomically tapered down to 1.5mm distally | Reduces flexor tendon irritation & attrition |
| Screw Thread Interface | Standard locking threads | Polyaxial/Variable angle locking (±15°) | Allows targeting of specific styloid fragments |
| Surface Treatment | Standard Anodization Type I | Type II Hard Anodization + Passivation | Enhances fatigue resistance and reduces galling |
Exploring a world-class production ecosystem built on rigorous testing, biomechanical simulation, and lean manufacturing.
Virelox Medical Devices Co., Ltd. is a professional orthopedic medical device manufacturer specializing in joint replacement and surgical implant solutions. Operating under the "Virelox" brand, the company delivers high-performance orthopedic systems for global healthcare providers, distributors, and surgical clinics.
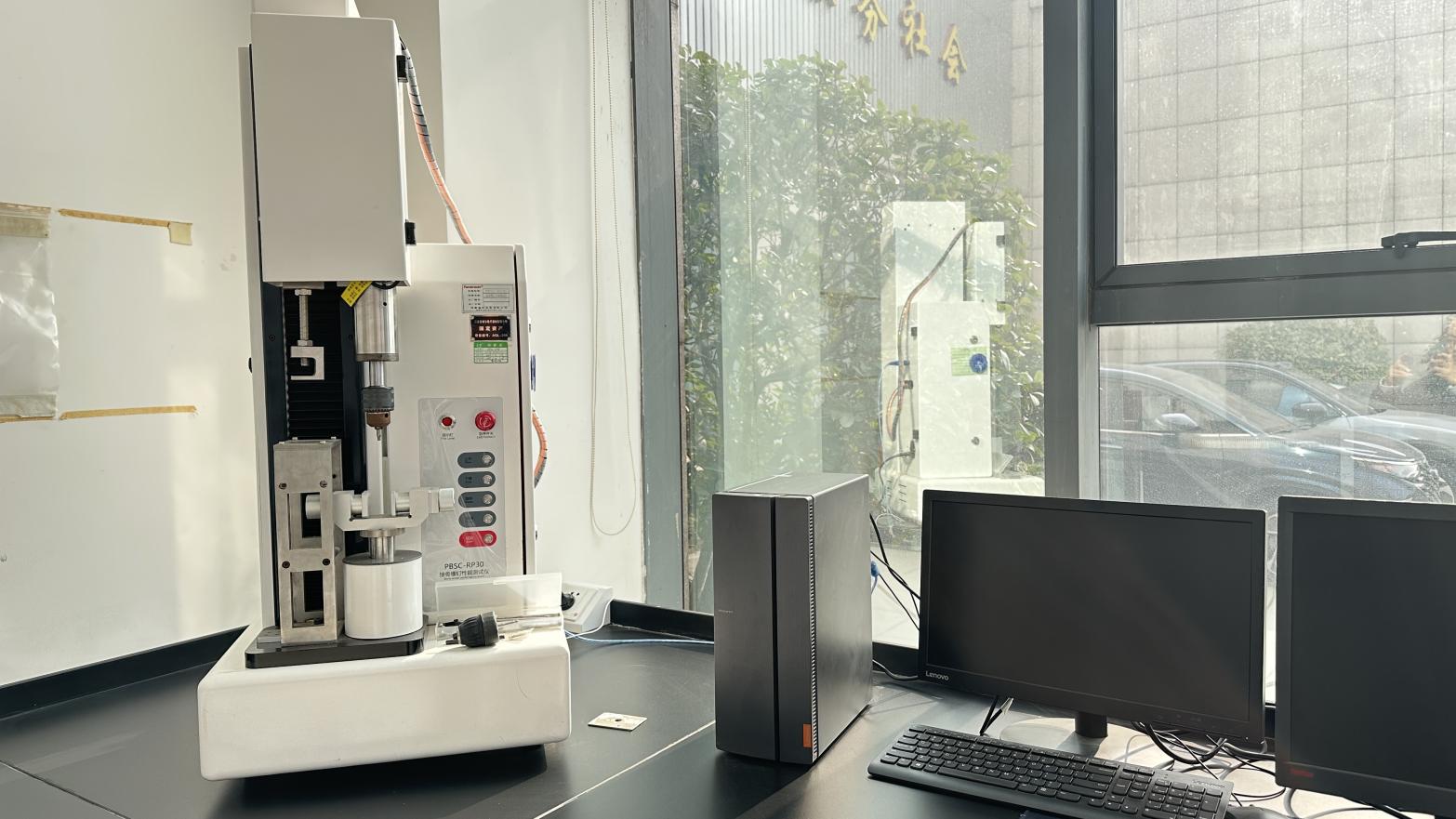
Each production stage is stringently monitored using advanced metrology, dimensional CMM, tensile systems, and fatigue testers.




















A comparative criteria framework for clinical buyers and procurement managers looking to minimize supply chain volatility.
When selecting a top-tier distal radius locking plate factory, buyers should evaluate companies based on these five pillars of operational capability:
Leading manufacturers provide mill run sheets and raw material certificates (e.g., medical-grade Ti6Al4V ELI conforming to ASTM F136). Material uniformity prevents catastrophic fatigue failure in vivo.
Cleanroom packaging areas operating under ISO Class 7 (Class 10,000) or ISO Class 8 conditions minimize bioburden and particulate contamination before final sterilization packaging.
Swiss-type longitudinal lathes and five-axis vertical machining centers keep geometric tolerances under 5 microns. This level of precision is necessary to guarantee secure screw-to-plate locking dynamics.
Evaluating the top 10 global suppliers requires reviewing their production volume, technological focus, and compliance track record. High-volume manufacturers leverage automated inspection processes to deliver cost savings, while specialized biomedical firms excel in custom anatomy plates and variable-angle polyaxial designs. The following guidelines represent the industry standard benchmarks used by leading distributors when performing factory audits in Asia and Europe.
How new materials and digital design integrations are shifting clinical paradigms in orthopedic traumatology.
Future systems focus heavily on polyaxial locking solutions. These allow surgeons to adjust screw trajectory within a 30-degree cone, helping them secure complex articular fragments without compromising the locking mechanism.
Developing anodized surface modifications (Type II) and silver/copper nanotechnology coatings helps reduce biofilm formation. These technologies speed up osseointegration and lower the risk of implant-associated infections.
Research is shifting toward high-strength magnesium-based alloys. These materials degrade safely inside the body after bone healing is complete, eliminating the need for a second surgery to remove the implant.
Detailed answers addressing technical queries, supply chain audits, and materials standards for clinical procurement teams.
Volar plates are positioned on the anterior surface of the radius, offering excellent anatomical support for most fractures with lower rates of extensor tendon irritation. Dorsal plates are reserved for complex dorsally displaced or intra-articular fractures, though they require low-profile designs to prevent extensor tendon complications.
Grade 5 ELI titanium alloy features a lower elastic modulus closer to human bone, which reduces stress shielding. It also provides superior fatigue resistance and biocompatibility, and produces fewer artifacts during MRI or CT imaging than stainless steel.
Variable-angle locking systems use a reinforced plate hole design paired with a hardened screw thread. This configuration allows the surgeon to angle the locking screw within a 15-degree radius (a 30-degree cone) to target specific bone fragments, while still maintaining stable locking mechanics.
Standard production cycles range from 45 to 60 days, depending on batch sizes and customization requirements. This timeline includes raw material testing, precision machining, passivation, inspection, and sterile packaging workflows.
Implants undergo rigorous dynamic fatigue testing under ASTM F382 or ISO 9585 standards. This testing subjects the plates to millions of cycles of bending stress to verify that they will perform reliably under actual anatomical loads.
Discover our comprehensive range of dynamic power tools, specialized spine systems, and repair instruments.